
Feeling a weird burning or zapping pain that just won’t quit? It might be nerve pain—and physio can actually help more than you think. In this blog, we’ll unpack what nerve pain really is, why it happens, and how physiotherapy can play a powerful role in calming things down.
What is Nerve Pain?
Nerve pain (also known as neuropathic pain) is one of those things that can really throw people. It’s different from the dull ache of sore muscles or the sharp stab of a sprain. It’s more like a burning, tingling, zapping, or electric shock kind of sensation. Sometimes it feels like your skin is overly sensitive. Other times, it’s like pain is coming from nowhere.
The most confusing part? The pain doesn’t always start where the problem is. For example, someone might feel pain in their foot, but the real issue could be up near the lower back or hip where the nerve is getting irritated.

Common Causes of Nerve Pain
Nerves can become irritated, compressed, or inflamed for a variety of reasons. Here are a few of the more common ones we see in clinic:
- Herniated discs: Pressure from a bulging disc can pinch a spinal nerve.
- Post-surgery changes: Scar tissue from surgery can sometimes irritate nearby nerves.
- Diabetes: Can lead to peripheral neuropathy, especially in the feet.
- Tight muscles: Believe it or not, tight muscles like the piriformis or hamstrings can entrap nerves like the sciatic or tibial nerve.
- Trauma: A direct hit or sudden stretch can irritate or even damage a nerve.
- Repetitive strain: Poor posture, long hours at a desk, or repeated movements can lead to chronic nerve irritation.

Symptoms to Watch Out For
If you’ve got nerve pain, you might notice:
- Burning or searing pain
- Pins and needles
- Tingling or numbness
- Weakness in a limb
- Shooting or zapping sensations down the arm or leg
- Sensitivity to touch (even clothes can feel painful)
Symptoms often follow the path of the affected nerve—so the location of pain can help us figure out which nerve is involved.

The Science Behind It: Why Nerves Hurt
Nerves are like the body’s communication cables. When one gets irritated, it starts sending distress signals. But here’s the thing—those signals don’t always make sense. The brain might interpret them as burning, zapping, or hypersensitivity.
Once a nerve becomes “sensitised”, it can become more reactive. This means it starts firing off pain signals even when there’s no actual danger. It’s like your body’s alarm system getting stuck on high alert.
How Physiotherapy Can Help with Nerve Pain
You might not think of physio as the go-to treatment for nerve pain—but it absolutely can be.
Here’s how we help:
1. Identify the Source
We don’t just treat the pain—we track down where it’s coming from. That might mean testing nerve mobility, looking at posture, assessing joint movement, and checking muscle tension.
2. Nerve Glides and Mobilisations
These gentle movements help the nerve slide and move more freely through its pathway. Think of it like flossing for your nerves—helping reduce tension and irritation.
3. Addressing the Root Cause
If the nerve is irritated because of a stiff joint, tight muscle, or poor biomechanics, we’ll treat that directly. This might involve hands-on therapy, stretching, strengthening, or movement retraining.
4. Postural Advice
Sometimes a simple change in how you sit or move during the day can reduce nerve tension and stop flare-ups.
5. Exercise Programming
Gradual, targeted strengthening helps support the body and reduce risk of future flare-ups. Plus, movement helps desensitise the nervous system over time.

Real Life Example: The Mysterious Burning Foot
We recently had a patient come in with a burning pain in their foot. They thought they must’ve kicked something or bruised it, but couldn’t remember doing so. The pain was constant, especially after walking or standing for long periods. Shoes made it worse. They described it as “like fire ants crawling on my foot.”
Assessment
We ruled out common things like plantar fasciitis, fractures, and local trauma. On testing, there was no obvious injury to the foot muscles or joints. But when we assessed nerve tension, we found the sural nerve was extremely sensitive.
The sural nerve runs down the back and outer part of the leg and ends near the heel and foot. Interestingly, this nerve can become irritated not just at the foot, but higher up, especially where it branches from the sciatic nerve.
Treatment
We started treatment not at the foot—but up around the sciatic nerve. We used nerve mobilisation techniques, soft tissue work to reduce tension in the hamstrings and glutes, and added some nerve gliding exercises to do at home.
Within a few sessions, the patient started noticing the burning was easing. After a couple of weeks, they could wear shoes again without pain. The best part? No injections or medication were needed—just good old-fashioned physio and a targeted plan.
Different Nerves, Different Pains
Depending on which nerve is involved, you might feel symptoms in different places. Here are a few common ones:
| Nerve | Typical Pain Area | Common Cause |
|---|---|---|
| Sciatic Nerve | Buttock, back of thigh, calf | Disc herniation, piriformis syndrome |
| Tibial Nerve | Bottom of foot, heel | Tarsal tunnel syndrome |
| Peroneal Nerve | Outer leg, top of foot | Fibular head compression |
| Sural Nerve | Outer lower leg, foot | Sciatic tension, tight calves |
| Median Nerve | Thumb, index, middle fingers | Carpal tunnel syndrome |
| Ulnar Nerve | Ring and little finger | Elbow compression (cubital tunnel) |
Knowing which nerve is involved helps us choose the right treatments—and avoid chasing the wrong problem.
How Long Does Nerve Pain Take to Settle?
This depends on:
- How long you’ve had the symptoms
- The severity of nerve irritation
- How sensitised the nervous system has become
- Whether you stick to your treatment plan
Some people feel relief in a few sessions. For others, especially if it’s been going on for months, it might take a bit longer. The key is consistency, patience, and not giving up.
What Can You Do At Home?
Here are a few self-care tips if you’re dealing with nerve pain:
- Avoid aggravating positions: Like prolonged sitting or crossing your legs if that makes it worse.
- Gentle nerve glides: Only if prescribed by your physio—these help restore normal nerve movement.
- Stay active: Light walking or swimming can help keep the nervous system happy.
- Don’t stretch too hard: Aggressive stretching can actually make nerve pain worse.
- Mind your posture: Especially if you work at a desk or spend hours in the car.
When to See a Physio
If you’re experiencing:
- Ongoing tingling, burning, or shooting pain
- Numbness or weakness in a limb
- Pain that doesn’t respond to basic rest or ice
- Pain that seems to travel or doesn’t make sense
…it’s time to book in.
We’ll do a thorough assessment, explain what’s going on in plain English, and put together a clear plan to help you feel normal again.
Final Thoughts
Nerve pain might feel scary and mysterious, but it’s often treatable without medication or surgery. Physiotherapists are trained to understand the nervous system, track down the source of your symptoms, and get you back to doing what you love.
Just like our patient with the burning foot—sometimes the pain is coming from somewhere you wouldn’t expect, and you just need the right treatment to unlock relief.
References
- Physiopedia. Neuropathic Pain
- Pain Australia. Neuropathic Pain
- British Journal of Sports Medicine. Nerve mobilisation for the treatment of pain
- Neuro Orthopaedic Institute. The Sensitive Nervous System
- Health Direct Australia. Nerve Pain
Want to know if nerve pain is behind your weird symptoms? Book an appointment today just CLICK HERE
Let us untangle your nerves (literally!).
Tried everything for tight muscles or stubborn pain and nothing seems to stick? Dry needling might just be the missing link. It’s fast becoming a favourite tool among physios for its deep, targeted relief. In this blog, we break down what it is, how it works, and why it could be a total game-changer for your recovery.
What Is Dry Needling?
Dry needling is a technique used by trained physiotherapists to treat muscle pain and dysfunction. It involves inserting very fine, sterile acupuncture needles into specific points in the muscles, often referred to as “trigger points” or tight bands. The goal? To release tension, improve blood flow, and reset dysfunctional movement patterns.
Now, before you think, “Isn’t that just acupuncture?” — let’s clear that up. While dry needling and acupuncture use similar needles, they’re based on entirely different principles. Acupuncture is rooted in traditional Chinese medicine and works along meridian lines and energy flow. Dry needling, on the other hand, is based on Western anatomy and targets the actual source of muscle dysfunction.

How Does It Work?
Dry needling works by creating a micro-lesion in the tissue that triggers a local twitch response — kind of like your muscle giving a little spasm. While that might sound odd, this twitch response is a good thing. It signals that the tight knot (trigger point) has been disrupted and the muscle is ready to let go.
Here’s what happens physiologically:
- Increased blood flow: Helps bring oxygen and nutrients to the area to promote healing.
- Decreased muscle tightness: By breaking up tight trigger points, the muscle returns to its normal length.
- Improved range of motion: You’ll often find you can move better straight after.
- Pain relief: By reducing tension and inflammation, many people report a noticeable reduction in pain.
Why We Use Dry Needling in Physiotherapy
At our clinic, dry needling is one of the most effective adjuncts to hands-on therapy and rehabilitation. It’s particularly helpful for:
- Chronic tightness within deeper muscles that massage alone can’t shift
- Sports injuries
- Neck and back pain
- Shoulder tension and rotator cuff problems
- Glute and hip tension
- Postural muscle imbalances
- Tension-type headaches
- We can use needles in the majority of muscles around the body
Dry needling allows us to “go deeper” into the muscle tissue than manual therapy can, which makes it a powerful tool in unlocking long-standing tightness and guarding patterns. It’s especially helpful when someone has hit a plateau with other treatments.

What Does Dry Needling Feel Like?
Let’s be honest — the idea of needles isn’t everyone’s cup of tea. But most people are surprised by how little it actually hurts. The needles are very thin — about the size of a hair — and don’t inject anything (hence the term “dry”).
You might feel a slight pinch when the needle goes in, and a twitch or dull ache if we hit a trigger point. But this usually lasts just a second or two and is followed by a feeling of release. Some people feel a bit sore afterwards — like a gym workout — but this settles quickly.
Is It Safe?
Absolutely — when done by a qualified practitioner. All our physios who use dry needling have undergone additional training and are registered with the Australian Health Practitioner Regulation Agency (AHPRA). We use sterile, single-use needles and follow strict hygiene protocols.
As with any treatment, there are small risks (e.g. bruising or temporary soreness), but serious complications are extremely rare. We’ll always talk you through it beforehand and make sure it’s suitable for your condition and comfort level.
Real Results: A Patient Story
Let’s take a look at how dry needling made a real difference for one of our recent patients — let’s call her Emma.
Emma is a 38-year-old graphic designer who had been dealing with ongoing shoulder and upper back pain for nearly three years. Her symptoms would flare up especially after long hours at her desk or during workouts. She’d tried everything: chiropractic adjustments, osteopathy, massage, and even seen three different physiotherapists. While each helped a bit, the relief never lasted.
When Emma came to us, she was understandably frustrated. Her muscles felt constantly tight, and no amount of stretching or massage seemed to shift it. After a thorough assessment, we identified some deep myofascial trigger points in her upper traps, rhomboids, and rotator cuff.
We introduced dry needling in her second session, targeting those deeper muscle layers that had been resistant to other treatments. Sarah felt an immediate difference — she described it as if someone had “hit the reset button” on her shoulder.
Over the next few sessions, we combined dry needling with hands-on therapy, posture retraining, and a targeted exercise program. With her muscles finally able to relax, we could strengthen her shoulder girdle and improve her movement patterns without triggering pain.
Three months later, Emma is back in the gym, sitting comfortably at her desk, and hasn’t needed to return for a flare-up. She even jokes that dry needling was the “missing ingredient” no one else had offered.
How We Incorporate It Into Treatment
Dry needling isn’t a one-size-fits-all solution — it’s a tool in a broader physio toolkit. At our clinic, we use it in a targeted, evidence-based way. That means:
- Thorough assessment to determine if needling is appropriate
- Clear explanation of what to expect
- Combining dry needling with rehab, manual therapy, and education
- Monitoring your response and adjusting treatment as needed
We usually don’t rely on dry needling as a standalone. It’s most effective when used alongside strengthening, mobility work, and lifestyle changes (like work set-up or sleep posture).

Who Shouldn’t Have Dry Needling?
While dry needling is safe for most people, there are a few situations where we’d hold off or approach with extra care. These include:
- People with a fear of needles or severe anxiety
- Pregnancy (especially in early stages)
- Bleeding disorders or people on blood thinners
- Certain medical conditions (e.g. uncontrolled diabetes, cancer)
If you’re not sure, just ask. We always tailor treatment to your individual needs and comfort level.
What Does the Research Say?
Dry needling is backed by a growing body of research, especially for musculoskeletal pain and trigger point release. Studies have shown that dry needling can:
- Reduce pain in both acute and chronic conditions
(Gattie et al., 2017) - Improve range of motion and muscle function
(Kietrys et al., 2013) - Be more effective than no treatment or placebo for trigger points
(Liu et al., 2015)
While not a miracle cure, dry needling is increasingly seen as a valuable adjunct in physiotherapy, particularly when traditional methods haven’t been enough.
FAQs
How many sessions will I need?
This really depends on the issue. Some people get big results in 1–2 sessions, while others may benefit from a short course alongside their rehab program.
Is it the same as trigger point massage therapy?
Similar idea — both target muscle knots. But dry needling uses a needle to go deeper, which can be more effective for stubborn trigger points.
Can I exercise after dry needling?
Yes, but we usually suggest light activity on the same day and heavier training the following day. You might feel a bit sore — that’s normal.
Do the needles stay in long?
Usually not. Most are inserted and removed within a few seconds. Sometimes we’ll leave them in for a few minutes depending on the area.
Final Thoughts
Dry needling might sound intense, but it’s actually a gentle and highly targeted way to release muscle tension that other techniques just can’t reach. If you’ve been stuck in a cycle of pain, especially with recurring tightness that just won’t let go, dry needling could be the breakthrough you need.
And remember — it’s not about “just needling and done.” It’s about using the right tools, in the right hands, at the right time.

References & Further Reading
- Gattie, E., Cleland, J., & Snodgrass, S. (2017). Dry needling versus sham needling for myofascial pain: A systematic review and meta-analysis. The Journal of Manual & Manipulative Therapy. Read here
- Kietrys, D. M., Palombaro, K. M., & Azzaretto, E. (2013). Effectiveness of dry needling for upper-quarter myofascial pain: A systematic review and meta-analysis. J Orthop Sports Phys Ther, 43(9), 620-634. Read here
- Liu, L., Huang, Q. M., Liu, Q. G., et al. (2015). Effectiveness of dry needling for myofascial trigger points associated with neck and shoulder pain: A systematic review and meta-analysis. Archives of Physical Medicine and Rehabilitation. Read here
- Australian Physiotherapy Association – Dry Needling in Physiotherapy
Let us know if you’re curious about whether dry needling could work for your condition — we’re always happy to chat! Call us on 9806 3077 today.
Scoliosis isn’t just a spine that’s a bit wonky — it can cause pain, stiffness, breathing issues, and knock-on effects throughout the body. But here’s the good news: with the right physiotherapy treatment, many people can feel stronger, move better, and regain confidence. Read on to find out how.
What Is Scoliosis?
Scoliosis is a condition where the spine curves sideways — often in an “S” or “C” shape — instead of running straight down the middle of the back. While a small curve may not cause much trouble, more significant curvatures can lead to pain, stiffness, posture changes, and sometimes even breathing difficulties if the rib cage is affected.
There are a few different types:
- Idiopathic scoliosis (most common in teens, cause unknown)
- Congenital scoliosis (due to bone abnormalities from birth)
- Neuromuscular scoliosis (linked to conditions like cerebral palsy or muscular dystrophy)
- Degenerative scoliosis (often found in older adults due to spinal wear and tear)
Scoliosis is more common than you might think, especially among teenagers going through growth spurts. In fact, according to the Research Society, idiopathic type affects around 2-3% of adolescents (SRS, 2023).

Spotting the Signs
Scoliosis can sneak up on you — it’s often painless at first. Many kids and teens don’t even realise they have it until it’s picked up during a Physiotherapy screening, or GP visit, or when a parent notices something “off.”
Here are a few tell-tale signs:
- Uneven shoulders or waist
- One shoulder blade sticking out more
- Ribs more prominent on one side when bending forward
- Clothes hanging unevenly
- Leaning to one side
In more serious cases, the spine rotation can affect how the ribs sit, leading to breathing difficulties, back pain, or fatigue during sport or physical activity.

How Is Scoliosis Diagnosed?
Diagnosis usually starts with a physical exam. Your GP or physio might do the “Adam’s Forward Bend Test” — where you bend forward from the waist, and they look for asymmetry in the ribs or back.
From there, imaging like X-rays or even an MRI can be used to confirm the curve and measure its severity. The angle is measured using something called the Cobb angle:
- Mild: < 20 degrees
- Moderate: 20–40 degrees
- Severe: > 40 degrees
The Cobb angle helps determine whether the angle is likely to worsen and what sort of treatment is recommended.

Treatment Options: It’s Not One-Size-Fits-All
Treatment depends on the type of scoliosis, the age of the person, and how far the curve has progressed. Here’s a breakdown:
1. Observation
In mild cases — particularly if the child is still growing — the doctor may simply monitor the curve over time with regular check-ups and X-rays. Physiotherapy is usually started at this point to strengthen muscles, improve posture and reduce any asymmetries in movement.
2. Bracing
If the curve is moderate and the child is still growing, a back brace might be recommended. The goal isn’t to reverse the curve, but to stop it from getting worse. It’s usually worn for 16–23 hours a day — not exactly fun for a teenager, but it can be effective.
3. Surgery
Surgery is generally considered when the curve is severe (> 45–50 degrees) and still progressing. The most common procedure is spinal fusion, where metal rods, screws and bone grafts are used to straighten and stabilise the spine.
But surgery isn’t the end of the road — far from it. That’s where physiotherapy steps in to play a huge role in recovery.

Physiotherapy: What We Actually Do
Whether someone’s managing the curvature of the spine conservatively or recovering from surgery, physio can make a big difference.
In non-surgical cases, we focus on:
- Postural correction
- Core strengthening
- Breathing techniques (for rib rotation or breathing restrictions)
- Stretching tight muscles
- Manual therapy to ease stiffness or pain
- Education on activity pacing and ergonomics
After surgery, physio helps with:
- Improving spinal mobility (within safe limits)
- Building strength in the core and back muscles
- Improving lung function (particularly if surgery affected the ribs)
- Restoring confidence with movement
- Getting back to sport or school activities

Jeremy’s Journey – A Case Study
Let’s talk about Jeremy, a 15-year-old student and keen swimmer who came to our clinic last year. His parents had noticed his posture seemed “off” and that he’d been complaining of a dull ache in his mid-back, especially after sport.
We did a postural assessment and referred him for imaging, which showed a 52-degree thoracic curve — classified as severe adolescent idiopathic scoliosis.
Due to the size of the curve and Jeremy’s age (he was still growing), a spinal surgeon was consulted. Jeremy underwent spinal surgery to correct the curve and prevent further progression.
He came to us about three weeks post-op. At that point, he was still stiff, cautious with movement, and had some weakness through his core and hips.
We created a rehab plan that included:
- Gentle mobility and breathing work
- Gradual core and glute strengthening
- Postural training and neuromuscular control
- A return-to-sport timeline that kept him moving without overloading
Jeremy worked hard. By 10 weeks post-op, he was confidently walking and doing bodyweight exercises. By six months, he was back playing modified soccer training drills — with medical clearance and a huge grin on his face.
Now, Jeremy pops into the clinic once a month for check-ins and continues a home program. He’s stronger, more confident, and pain-free — a great example of what’s possible when surgery and physiotherapy work hand-in-hand.
What About Adults With Scoliosis?
While most people associate scoliosis with teenagers, adults can develop it too. Often it’s due to spinal degeneration (called degenerative scoliosis), especially in people over 50.
Symptoms might include:
- Low back pain
- Leg pain from nerve irritation
- Changes in posture
- Fatigue with walking or standing
Treatment for adults usually focuses on pain relief, improving flexibility and strength, and reducing pressure on irritated nerves.

Exercise and Scoliosis: What Works?
A lot of people with scoliosis are told to avoid certain exercises or feel nervous about movement. But we now know that a well-structured exercise program — especially guided by a physio — can be hugely beneficial.
Some great options include:
- Pilates (especially clinical Pilates with a physio)
- Swimming (non-weight bearing and helps posture)
- Yoga (modified poses that avoid deep backbends or side bending)
- Strength training (especially core, glutes, and back)
We’ll always tailor exercises to the person’s needs, making sure it’s safe and effective. For someone like Jeremy, it was important to avoid twisting and high-impact exercises early on — but over time, we added agility drills and soccer-specific movements.

Common Myths About Scoliosis
Let’s bust a few common scoliosis myths:
🚫 “Scoliosis is caused by bad posture.”
Nope — especially idiopathic scoliosis, which has no known cause.
🚫 “Only girls get scoliosis.”
Girls are more likely to have curves that worsen, but boys can get it too.
🚫 “Scoliosis always leads to pain or disability.”
Not true — many people with scoliosis live full, active, pain-free lives.
🚫 “Surgery fixes everything instantly.”
Surgery can help correct the curve, but physio plays a key role in recovery and long-term function.
When to See a Physio
If you or your child has been diagnosed with scoliosis — or if you’re just not sure — seeing a physio early can make a real difference. We can assess posture, identify muscle imbalances, build strength, and help prevent progression or complications.
We also work closely with GPs, orthopaedic surgeons, and paediatricians to coordinate care when needed.
If you have any questions give us a call today on 9806 3077.
Final Thoughts
Scoliosis can seem scary at first, especially for teens like Jeremy who suddenly find themselves facing big changes to their body. But with the right guidance, support, and a solid physio plan, most people can move well, stay active, and feel confident again — whether surgery is part of the journey or not.
Movement really is powerful. And at the end of the day, that’s what physiotherapy is all about — helping you move better, feel stronger, and live life your way.
References and Further Reading
- Scoliosis Research Society. Adolescent Idiopathic Scoliosis
- Better Health Channel (Vic Gov). Scoliosis
- Australian Physiotherapy Association. How physios help with scoliosis
- Schroth Method info from Scoliosis and Spine Online Learning (SSOL). https://scoliosisandspineonlinelearning.com/
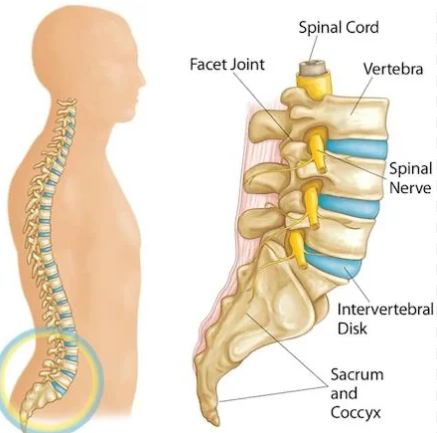
Back pain is ridiculously common and can really throw a spanner in the works when it comes to work, sleep, and everyday life. But the good news? Most cases improve significantly with targeted physiotherapy. In this blog, we’ll unpack the different causes of back pain, the role of physio, and share a real case of one of our patients who bounced back from a facet joint sprain.
Back Pain – Why Is It So Common?
Back pain is one of the most frequent complaints we see in the clinic. In fact, around 80% of Aussies will experience back pain at some point in their lives (Australian Institute of Health and Welfare, 2023). It doesn’t discriminate—office workers, tradies, new mums, and athletes alike can all be affected.
For some people, it’s a dull, nagging ache that’s always there. For others, it’s a sharp, take-your-breath-away type of pain that can stop you in your tracks. It can come on suddenly (like after lifting something the wrong way), or sneak up slowly after years of poor posture, stress, and weak core muscles.
But here’s the key message: most back pain is not serious, and it’s treatable.

The Usual Suspects – Common Causes of Back Pain
Let’s break down a few of the more common culprits:
1. Facet Joint Sprains
These small joints at the back of the spine help with movement and stability. They can become inflamed or irritated, especially after awkward lifting, twisting, or prolonged poor posture.
2. Disc Issues
Things like disc bulges or herniations can press on nearby nerves, causing pain that radiates into the legs (commonly known as sciatica).
3. Muscle Strains
This is your typical “I bent down and felt something go” moment. Muscle spasms and tightness are often part of the picture.
4. Poor Posture
Spending too much time hunched over a desk or slouched on the couch can strain the muscles and joints in your back.
5. Stress and Tension
Believe it or not, emotional stress can tighten muscles and amplify pain signals.
Red Flags – When to See a Doctor ASAP
While most back pain is manageable, some signs need urgent medical review:
- Numbness in the groin area
- Loss of bladder or bowel control
- Sudden weakness in the legs
- History of cancer or recent unexplained weight loss
If you’re experiencing any of the above, don’t muck around—see your GP.
The Role of Physiotherapy in Treating Back Pain
Physiotherapists are experts in assessing, diagnosing, and treating musculoskeletal pain—including back pain. At our clinic, we don’t just hand you a list of exercises and send you on your way. We dive into what’s really going on, and more importantly, why.
Here’s how we help:
1. Thorough Assessment
We take a detailed history, check your movement, palpate structures, test muscle strength, and sometimes assess nerve involvement.
2. Hands-On Treatment
This might include joint mobilisation, soft tissue release, dry needling, taping, or spinal manipulation (where appropriate).
3. Targeted Exercise Program
Not a generic YouTube routine! We tailor your program to improve your flexibility, strength, and control—especially around the hips, core, and lower back.
4. Education
Understanding your pain is half the battle. We help you make sense of your symptoms, which often reduces fear and anxiety.
5. Lifestyle Modifications
We look at your work setup, sleep position, activity levels, and stress—all of which can influence recovery.

Patient Case Study: Dylan’s Facet Joint Sprain
Let’s look at a real example from our clinic. Dylan (not his real name), a 42-year-old carpenter, came in with acute lower back pain after lifting a heavy timber frame at work. He’d felt a sharp pinch and then seized up. By the time he got to us, he was struggling to bend, had pain turning over in bed, and couldn’t drive for more than 10 minutes without discomfort.
Initial Assessment
Our assessment pointed to a facet joint sprain. He had tenderness over the joints in the lower lumbar spine, reduced extension, and a classic “catch” when returning to upright from bending forward.
We also ruled out red flags and any signs of nerve compression—his leg strength and sensation were all normal, and there was no sciatic-type pain.
Treatment Plan
We got to work straight away. His program included:
- Manual therapy – gentle joint mobilisations and soft tissue release around the lower back and glutes
- Taping – to support the lumbar area and reduce strain
- Dry needling – for deep muscle spasm
- Education – reassuring Mark that he hadn’t “done his back in” permanently
- Exercise – starting with basic pelvic tilts, glute bridges and breathing control, then progressing to strengthening through range
Within three sessions, Dylan had significantly improved. By week 4, he was back on-site, modified duties at first, and by week 6, he was moving better than before the injury. He’s now working on long-term spinal strength with our gym program to help bulletproof his back.
What About Scans?
You might be surprised to learn that scans are often unnecessary for back pain—especially early on. Many people with scary-sounding scan results (like disc bulges or degeneration) have no pain at all. And on the flip side, someone with severe pain might have completely normal imaging.
Unless we see red flags or symptoms that persist beyond 6 weeks despite treatment, we usually don’t rush for MRIs or CTs. Instead, we focus on your movement, function, and pain response.

What Can You Do at Home?
While it’s always good to get properly assessed, there are some general tips to help manage back pain in the early stages:
✅ Keep Moving
Bed rest is out, gentle movement is in. Even walking around the block can help keep things from stiffening up.
✅ Heat or Ice
Whichever feels better—some people love heat packs, others swear by ice. Try both and see what works for you.
✅ Gentle Stretching
Think of movements like cat-cow, child’s pose, or lying knee rocks. Nothing too aggressive—just enough to stay mobile.
✅ Avoid Sitting Too Long
If you’re stuck at a desk, set a timer every 30–60 minutes to get up, stretch, and move.
✅ Stay Positive
Back pain can be annoying and scary, but most cases settle well with the right approach.

How Long Does Recovery Take?
It depends on the cause and your overall health. Acute mechanical back pain (like Dylan’s) often settles within 4–6 weeks. More chronic or recurrent cases can take longer, especially if deconditioning or poor movement habits are part of the picture.
The goal of physio isn’t just to get you out of pain—it’s to keep you there by building resilience and control.
Prevention – Can You Stop It Coming Back?
Absolutely! Here are our top 5 prevention tips:
- Strengthen Your Core This doesn’t mean endless sit-ups—think planks, glute work, and dynamic control exercises.
- Lift Properly Bend your knees, keep the load close to your body, and avoid twisting while lifting.
- Workstation Setup Desk workers—make sure your chair, monitor, and keyboard are set up properly to reduce strain.
- Stretch Regularly Especially through your hips and hamstrings—they can pull on your back if tight.
- Stay Active Regular walking, swimming, Pilates, or gym work is great for spinal health.

Final Thoughts
Back pain is common, but it’s also treatable. Whether it’s a one-off strain or something that’s been hanging around for years, physiotherapy can make a real difference.
If you’re battling with a cranky lower back, don’t tough it out alone. Book in with one of our physios and let’s get to the bottom of it (literally and figuratively).
References & Further Reading
- Australian Institute of Health and Welfare. (2023). Back problems.
- Physiopedia. Facet Joint Syndrome.
- Better Health Channel. (n.d.). Back pain.
- Spine-Health. When You Should Worry About Low Back Pain.
- Blog: What Is a Facet Joint Sprain?
- Blog: How to Strengthen Your Core Without Hurting Your Back
Athlete screening is like a pre-season tune-up for your body—identifying weaknesses, imbalances, and risks before they turn into injuries. Whether you’re a weekend warrior or an elite competitor, screening helps tailor training and rehab programs to keep you performing at your best. In this blog, we’ll dive into why screenings matter, what they involve, and a real-life case study showing their impact.
What is Athlete Screening?
Athlete screening is a structured assessment that identifies potential injury risks, biomechanical inefficiencies, and performance limitations. It’s commonly used in pre-season evaluations across various sports, from soccer to swimming. The goal is to detect imbalances or weaknesses that could lead to injury if left unaddressed.
A thorough athlete screening includes:
- Strength testing (e.g., single-leg squats, calf raises)
- Flexibility and mobility assessments
- Balance and proprioception tests
- Functional movement screening (FMS)
- Sport-specific drills (e.g., sprint mechanics, jump landing techniques)

Why is Athlete Screening Important?
Many injuries don’t happen suddenly—they build up over time due to poor movement patterns, muscle imbalances, or inadequate strength in key areas. A screening helps:
- Prevent injuries – By identifying weak links before they lead to strains or sprains.
- Enhance performance – A more balanced and efficient body moves faster, jumps higher, and endures longer.
- Customise training plans – Targeted rehab or strength programs address individual needs.
- Boost longevity in sport – Reducing injury risk means more seasons of play.

The Screening Process: What to Expect
During a screening, a physiotherapist assesses different movement patterns and strength levels. The process typically includes:
1. Medical and Injury History
We discuss past injuries, recurring pain, and any areas of concern. This helps tailor the screening process.
2. Strength and Stability Tests
Muscle strength is assessed through controlled exercises like single-leg squats, push-offs, and resistance-based tests.
3. Flexibility and Mobility Checks
Tight hamstrings, limited ankle dorsiflexion, or stiff hip flexors can all contribute to injury risk.
4. Functional Movement Analysis
Using techniques like the Functional Movement Screen (FMS), we observe how an athlete moves, squats, lunges, and pivots.
5. Sport-Specific Testing
For soccer players, this might involve cutting movements, balance while striking the ball, or sprint mechanics.

Case Study: Screening Saves a Soccer Season
Recently, we screened a 19-year-old soccer player ahead of their upcoming season. They had a history of minor ankle sprains but no major injuries. During the screening, we noticed something crucial: a significant weakness in their left calf.
Key Findings:
- The player struggled to complete the same number of single-leg calf raises on the left side as on the right.
- Balance on the left leg was noticeably weaker.
- Sprint acceleration showed a slight asymmetry, indicating a potential performance deficit.
- The player explained they had sprained their ankle in the last game of last season but did not do any rehabilitation in the off season.
The Solution:
We in designed a six-week rehab program to strengthen the left calf and improve overall lower limb stability. The plan included:
- Calf raises (both bent and straight knee) – 3 sets until fatigue
- Single-leg balance drills to enhance proprioception
- Eccentric calf strengthening exercises
- Progressive plyometrics to improve explosive power
The Result:
By the start of the season, the athlete reported feeling stronger and more balanced. They completed the pre-season without any sprains, improved their sprinting mechanics, and felt more confident in their cutting movements.
Who Should Get Screened?
Athlete screening isn’t just for professionals. If you:
- Have had a previous injury and want to prevent a recurrence
- Experience niggling pain that comes and goes
- Want to improve performance by identifying movement inefficiencies
- Play a high-impact sport like soccer, basketball, AFL, rugby union
Then a pre-season screening could be a game-changer for you.

Final Thoughts
Athlete screening is an investment in your body and performance. Whether you’re recovering from an injury or aiming to prevent one, understanding your strengths and weaknesses can help you train smarter. If you’re heading into a new season, now is the perfect time to book a screening and stay ahead of injuries!
References & Further Reading:
- Functional Movement Systems. (n.d.). What is FMS? https://www.functionalmovement.com
- Sports Medicine Australia. (n.d.). Injury prevention strategies for athletes. https://sma.org.au
- FIFA 11+. (n.d.). A complete warm-up program for injury prevention in soccer. https://www.fifamedicalnetwork.com
Ready to get screened? Contact us today to book your athlete screening session!
Introduction Hypermobility might sound like a superpower, but for many people, it’s a hidden struggle. Loose joints can lead to pain, fatigue, and even injuries. But here’s the good news—physiotherapy can make a massive difference. In this blog, we’ll break down what hypermobility is, why it happens, and how targeted physio treatment can help you stay strong and pain-free.
What is Hypermobility?
Hypermobility refers to excessive movement in the joints due to looser connective tissues. Some people are naturally more flexible, but when the increased flexibility causes pain, instability, or repeated injuries, it becomes a medical concern. This is often referred to as Joint Hypermobility Syndrome (JHS) or, in more severe cases, Ehlers-Danlos Syndrome (EDS).
Common complaints:
- Frequent joint pain, especially after activity
- Increased risk of sprains, dislocations, and joint injuries
- Fatigue due to muscles working harder to stabilise joints
- Poor proprioception (awareness of body position)
- Digestive issues, dizziness, and other systemic symptoms in cases of EDS
Why Does Hypermobility Happen?
Hypermobility is largely genetic. The main culprit? Collagen. This vital protein gives connective tissues their structure and strength. When collagen is more elastic than normal, joints become extra flexible but also unstable. Other contributing factors include:
- Hormones – Oestrogen can influence tissue laxity, which is why hypermobility symptoms often worsen during pregnancy or hormonal changes.
- Muscle Weakness – Weak stabilising muscles allow joints to move excessively.
- Poor Motor Control – The brain struggles to sense and control joint positions, increasing the risk of injury.

How Physiotherapists Assess for Hypermobility
Physiotherapists use a range of tests to assess joint hypermobility and determine its impact on function. One of the most widely used tools is the Beighton Score, which helps quantify joint laxity.

Beighton Score Assessment
The Beighton Score is a 9-point scale assessing hypermobility at five different joint areas:
- Ability to bend the pinky finger back beyond 90 degrees (1 point per hand)
- Ability to touch the thumb to the forearm (1 point per hand)
- Hyperextension of the elbows beyond 10 degrees (1 point per elbow)
- Hyperextension of the knees beyond 10 degrees (1 point per knee)
- Ability to place palms flat on the floor with straight legs (1 point)
A score of 5 or more (out of 9) suggests generalised joint hypermobility, though clinical judgement is needed to assess its significance.
Additional Assessment Techniques
- Functional Movement Analysis – Observing movement patterns during tasks like squatting, walking, and reaching.
- Strength and Stability Tests – Checking for muscle control around hypermobile joints.
- Proprioception Tests – Assessing balance and joint position awareness.
- Pain and Fatigue Questionnaires – Understanding the broader impact of hypermobility on daily life.
This thorough assessment helps physiotherapists create individualised treatment plans tailored to each patient’s needs.
How Physiotherapy Helps Hypermobility
Physiotherapy plays a crucial role in managing hypermobility by strengthening muscles, improving proprioception, and reducing pain. Here’s what physios focus on:
1. Strengthening & Stability Training
Strength training is essential to help stabilise loose joints. The goal isn’t just to build muscle but to train the right muscles to activate at the right time.
- Core stability work – Stronger core muscles help protect the spine and prevent excessive movement.
- Glute activation exercises – Essential for hip and knee stability.
- Shoulder stability drills – Helps reduce dislocations in hypermobile shoulders.

2. Proprioception & Motor Control Training
Since hypermobile individuals often struggle with joint position awareness, physios use:
- Balance exercises – Like single-leg stands or wobble board training.
- Closed-chain exercises – Movements with feet or hands in contact with the ground to improve stability.
- Neuromuscular training – Teaching the brain to better control movement and prevent injuries.
3. Pain Management Strategies
Pain in hypermobility isn’t always from injury—it’s often from muscle overuse and poor joint alignment. Physios use:
- Soft tissue techniques – To relieve muscle tightness.
- Taping and bracing – Provides extra joint support during activity.
- Activity modification – Finding the right balance between movement and rest.

4. Education & Lifestyle Advice
Education is a huge part of treatment. Physios teach:
- How to move efficiently without overloading joints.
- When to rest vs. push through discomfort.
- The importance of proper footwear and ergonomic setups for daily life.
A Recent Success Story: Meet Sophie
Sophie, a 26-year-old yoga instructor, came to the clinic with chronic knee pain and frequent shoulder subluxations (partial dislocations). Despite being incredibly flexible, she struggled with strength and stability, making everyday activities exhausting.
During her physio sessions, we focused on glute and core strengthening, shoulder stability drills, and proprioceptive training to improve her joint control. We also adjusted her yoga practice to avoid overstretching vulnerable joints. After 12 weeks, Sophie reported significantly less pain, fewer dislocations, and more confidence in her body’s ability to move safely. She’s now back to teaching yoga but with a much smarter approach to her own movement.
Can You Prevent Hypermobility Issues?
While you can’t change your genetics, you can absolutely reduce the impact of hypermobility on your life. Here’s how:
- Strength train regularly – Focus on controlled movements, not just flexibility.
- Warm up properly – Avoid static stretching before exercise; opt for dynamic warm-ups instead.
- Listen to your body – If an activity causes pain or excessive fatigue, modify it.
- Seek professional advice – A physio can help tailor an exercise program specific to your needs.
Final Thoughts
Hypermobility doesn’t have to mean constant pain or injury. With the right physiotherapy approach, you can build strength, stability, and confidence in your movement. If you struggle with joint pain or instability, book a physiotherapy session and take control of your health today! Give us a call on 9806 3077 today to ask more about your injury.
References & Further Reading
- National Health Service (NHS). (2024). Hypermobility and Joint Hypermobility Syndrome. Retrieved from: https://www.nhs.uk/conditions/hypermobility/
- Ehlers-Danlos Society. (2024). Understanding Hypermobility. Retrieved from: https://www.ehlers-danlos.com/
- Australian Physiotherapy Association (APA). (2024). Physiotherapy and Joint Hypermobility. Retrieved from: https://australian.physio/
Looking for more physio insights? Check out our other blogs on joint health, strength training, and injury prevention!
Pilates isn’t just about core strength—it’s a game-changer for rehabilitation, injury prevention, and overall movement quality. Whether you’re recovering from an injury or just want to move better, both reformer and mat Pilates can help. In this blog, we’ll break down the benefits, differences, and how Pilates can be integrated into physiotherapy to fast-track your recovery.
What Is It?
Pilates is a form of low-impact exercise designed to improve flexibility, strength, and body awareness. Created by Joseph Pilates in the early 20th century, it has since evolved into a widely used approach in fitness and rehabilitation settings. It focuses on core control, alignment, and fluid movement, making it a go-to for physiotherapists working with patients recovering from injury or managing chronic conditions.
There are two main types:
- Mat: Uses body weight and small props like resistance bands or stability balls.

- Reformer: Uses a specialised machine with springs and pulleys to add resistance and support movements.

Why Physiotherapists Love It
Physiotherapists often incorporate Pilates into rehabilitation programs because it targets key muscle groups without overloading injured tissues. Key benefits include:
- Core Activation: Strengthens deep abdominal and spinal muscles, crucial for posture and back health.
- Joint Stability: Improves balance and reduces the risk of re-injury.
- Low-Impact Strengthening: Perfect for those recovering from surgery or injury.
- Enhanced Flexibility: Aids in movement efficiency and reduces stiffness.
- Mind-Body Connection: Encourages better movement patterns and control.
Reformer vs. Mat: Which One’s for You?
Both styles offer great benefits, but they have key differences:
| Feature | Reformer | Mat |
| Equipment | Uses a reformer machine with adjustable resistance | Uses a mat and small props like bands and balls |
| Support & Resistance | Offers assistance for controlled movement or resistance for strength-building | Relies on body weight and gravity for resistance |
| Best For | Injury rehab, strength building, and controlled movement | Core control, flexibility, and functional movement |
| Accessibility | Requires access to a reformer machine (usually in a clinic or studio) | Can be done anywhere with a mat |
Common Pilates Exercises for Rehabilitation
Mat Exercises
- Banded Bridging: Lying on your back with a resistance band around your thighs, lifting the hips while keeping knees in line to activate glutes and core.
- Dead Bug: Lying on your back, moving opposite arm and leg while keeping your core engaged.
- Single Leg Stretch: Alternating legs in a controlled motion while engaging the deep core muscles.
- Side-Lying Clams: Strengthens the hip stabilisers to improve knee and lower back function.
- Roll-Up: A slow, controlled movement to strengthen the core and improve spinal flexibility.
Reformer Exercises
- Reformer Leg Press: Lying on the reformer carriage, pressing against the foot bar to build lower limb strength and control.
- Footwork Series: Using different foot placements to target various muscle groups in the legs and feet.
- Seated Arm Work: Using the reformer’s pulleys for controlled upper body strengthening.
- Long Stretch Series: Engages core muscles while performing a controlled push-up motion on the reformer.
- Short Spine Exercise: A gentle way to mobilise the spine while engaging deep core muscles.
How Pilates Helps in Physiotherapy
1. Rehabilitation After Injury
It can be a fantastic rehabilitation tool for conditions such as:
- Lower back pain
- Post-surgical recovery (e.g., knee or hip replacements)
- Shoulder injuries (e.g., rotator cuff tears)
- Chronic pain conditions like osteoarthritis

2. Improving Posture & Reducing Pain
Many injuries and chronic pain issues stem from poor posture and muscle imbalances. It can help correct these imbalances by:
- Strengthening weak muscles
- Improving spinal alignment
- Enhancing body awareness
3. Enhancing Athletic Performance
Athletes use Pilates to prevent injuries and optimise performance. Sports like running, swimming, and soccer require core strength and joint stability—both of which can be benefits.

4. Managing Chronic Conditions
For those with long-term conditions such as:
- Osteoporosis (Pilates can help improve bone density and balance)
- Parkinson’s disease (focuses on controlled movement and coordination)
- Hypermobility syndromes (strengthens stabilising muscles)

Case Study: Overcoming Chronic Back Pain with Reformer Pilates
Meet Julie (name changed for privacy), a 42-year-old office worker who came to our clinic with persistent lower back pain. She had tried traditional physiotherapy exercises before but found it hard to maintain consistency.
After a thorough assessment, we introduced her to reformer, focusing on core strengthening and postural control. Within four weeks, she noticed a significant improvement in her back pain, mobility, and confidence in movement. Now, she attends weekly sessions to keep her back strong and pain-free.
Getting Started
If you’re recovering from an injury or want to improve your strength and mobility, Pilates could be a great addition to your rehab plan. At our clinic, we offer both mat and reformer Pilates under the guidance of experienced physiotherapists, ensuring safe and effective exercise tailored to your needs.
Watch Reformer Pilates in Action
For an example of a reformer session, check out this video: Reformer Pilates Example
Final Thoughts
Pilates isn’t just a workout—it’s a movement system that enhances recovery, strengthens the body, and promotes long-term health. Whether you’re new to it or looking to refine your technique, incorporating it into your physiotherapy plan can be a game-changer. We offer clinical pilates in our clinic at XPhysio Frenchs Forest. If you are curious, give us a call today on 9806 3077.
References
- Australian Physiotherapy Association. (2023). Pilates in Physiotherapy Rehabilitation. Retrieved from https://australian.physio
- Pilates Foundation Australia. (2023). Benefits of Pilates for Injury Recovery. Retrieved from https://www.pilatesfoundation.com.au
- Joseph Pilates. Return to Life Through Contrology. 1945.
Dizziness can be a frustrating and even scary experience. Whether it’s a sudden spinning sensation, a feeling of unsteadiness, or general light-headedness, dizziness can interfere with daily life. The good news? Physiotherapists are trained to assess and treat the various types, including vertigo, to help you regain balance and confidence.
In this blog, we’ll explore how physiotherapy can help with dizziness, the different types that can be treated, and a real-life case of a patient who improved with physiotherapy.
Types of Dizziness Physiotherapists Can Assess and Treat
Dizziness isn’t just one condition—it’s a symptom with multiple causes. Physiotherapists can assess and treat:
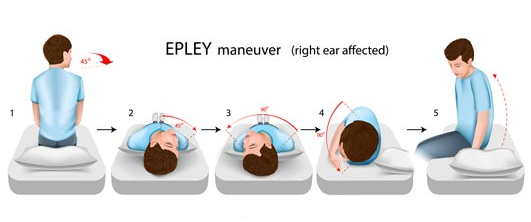
1. Benign Paroxysmal Positional Vertigo (BPPV)
BPPV is one of the most common causes of vertigo. It occurs when tiny calcium crystals in the inner ear become dislodged and move into the wrong canal. This leads to brief but intense episodes where the world feels as though it is spinning. It is often triggered by head movements, such as rolling over in bed or looking up.
Physiotherapy treatment:
- Canalith repositioning manoeuvres (e.g., the Epley manoeuvre) to move the dislodged crystals back where they belong.
- Education on how to manage symptoms and avoid provoking movements until the issue is resolved.
2. Cervicogenic Dizziness
This type originates from the neck and is often linked to poor posture, neck stiffness, or injury (e.g., whiplash). People with cervicogenic dizziness often report feeling unsteady or “off-balance” rather than experiencing true vertigo.
Physiotherapy treatment:
- Hands-on treatment for neck stiffness and muscle tightness.
- Postural correction and strengthening exercises.
- Balance retraining to improve stability.

3. Concussion-Related Dizziness
It is a common symptom following a concussion. It may be due to vestibular dysfunction, neck issues, or visual disturbances.
Physiotherapy treatment:
- Vestibular therapy to improve gaze stability and balance.
- Neck treatment if cervicogenic is present.
- Graded return-to-activity programs to ensure safe recovery.

A Recent Patient Case: Overcoming Cervicogenic Dizziness with Physiotherapy
Let’s look at a real-life example of a patient who was able to improve with physiotherapy.
Meet Sarah (name changed for privacy)
Sarah, a 42-year-old office worker, came into our clinic complaining of persistent dizziness that had been affecting her for months. She described it as a “floating” sensation rather than true spinning vertigo. It was worse after long hours at her desk and when she turned her head too quickly. She had seen a GP and undergone tests, but everything came back clear.
Assessment and Diagnosis
After a thorough assessment, we identified that Sarah’s symptoms were cervicogenic in nature—meaning it stemmed from her neck. She had significant muscle tightness in her upper neck, poor posture from long hours at her desk, and limited neck movement.
Physiotherapy Treatment
Sarah’s treatment plan included:
- Manual therapy: Hands-on techniques to release tight neck muscles and improve joint mobility.
- Postural correction: Exercises to strengthen her postural muscles and reduce strain on her neck.
- Balance retraining: Specific exercises to improve her stability and reduce her dizziness episodes.
- Education: Advice on workplace ergonomics and strategies to prevent recurrence.
Outcome
After four weeks of physiotherapy, Sarah reported a significant reduction in her dizziness. She felt more stable, her neck was moving more freely, and she could work without constant discomfort. With ongoing exercises, she was able to return to normal activities without the symptoms interfering in her life.
How to Know if Physiotherapy Can Help
If you experience dizziness, a physiotherapy assessment can help determine the cause. Physiotherapists use specific tests to differentiate between vestibular, neck-related, or other causes.
You may benefit from physiotherapy if you:
- Have your symptoms triggered by head or neck movements.
- Feel unsteady when walking or changing positions.
- Have a history of neck stiffness, poor posture, or recent injury.
- Experience lingering symptoms after a viral illness or concussion.

Final Thoughts
We know it can be frustrating, but you don’t have to live with it. Physiotherapists are well-equipped to assess and treat various forms of dizziness, from BPPV to cervicogenic dizziness. If you have symptoms described in this blog, a physio appointment could be the first step towards feeling steady and confident again.
References and Further Reading
- Better Health Channel. (n.d.). Dizziness and Vertigo. Retrieved from https://www.betterhealth.vic.gov.au
- Vestibular Disorders Association. (n.d.). Vestibular Rehabilitation Therapy. Retrieved from https://vestibular.org
- Physiopedia. (n.d.). Cervicogenic Dizziness. Retrieved from https://www.physio-pedia.com
- Mayo Clinic. (n.d.). Benign Paroxysmal Positional Vertigo (BPPV). Retrieved from https://www.mayoclinic.org
Book an appointment with XPhysio today on 9806 3077!
Bone fractures are a painful yet common injury that can happen to anyone, from kids on the playground to athletes and older adults. Whether it’s a simple wrist fracture from a fall or a more severe break requiring surgery, proper rehabilitation is essential for a full recovery. This is where physiotherapy plays a crucial role in getting you back to your normal life. In this blog, we’ll dive into what bone fractures are, how they heal, and how physiotherapy can speed up the recovery process.
What is a Bone Fracture?
A bone fracture occurs when there is a break in the continuity of the bone. Bone Fractures vary in severity and can be caused by trauma (such as a fall or car accident), repetitive stress (common in athletes), or medical conditions like osteoporosis that weaken bones.
Types of Bone Fractures
Bone Fractures come in different shapes and sizes, including:
- Closed (simple) fracture – The bone is broken but the skin remains intact.
- Open (compound) fracture – The bone breaks through the skin, increasing infection risk.
- Greenstick fracture – A partial break common in children due to softer bones.
- Comminuted fracture – The bone shatters into multiple pieces.
- Stress fracture – A small crack in the bone, often from overuse in sports.
- Pathological fracture – Caused by a disease that weakens bones, such as osteoporosis.
How Do Fractures Heal?
Healing a bone fracture is a complex process that occurs in several stages:
- Inflammation Phase (0-5 days) – The body responds to the injury with swelling and clot formation.
- Repair Phase (1-6 weeks) – New bone tissue, called callus, begins to form around the fracture site.
- Remodelling Phase (6 weeks – several months) – The new bone strengthens and reshapes to restore its original structure.
Healing time depends on factors like age, overall health, and the type of bone fracture. Children tend to heal faster than adults, while bone fractures in weight-bearing bones (like the femur) may take longer.
Expert Fracture Management at Our Clinic
Our physiotherapists are highly experienced in bone fracture management and can assist from the moment the injury occurs. We are able to fit a range of devices to protect and support the fracture, including:
- Cam walkers and moon boots to immobilise lower limb fractures while allowing some mobility.
- Rigid sandals for forefoot fractures to provide stability.
- Joint immobilising braces that function similarly to casting but allow for some flexibility in treatment.
- Splints for wrist and finger fractures to ensure proper positioning during healing.
- Crutches fitting and gait training to offload the affected area and promote a safe recovery.
By addressing the fracture immediately with the right support, we help minimise complications and ensure a smoother recovery process.

Why Physiotherapy is Essential for Fracture Recovery
While bones heal naturally, physiotherapy helps ensure they heal correctly and that you regain full function. Here’s how physio plays a key role in your recovery:
1. Reducing Stiffness and Swelling
After a fracture, joints around the injury often become stiff due to immobilisation (such as being in a cast or splint). Physiotherapy includes gentle movements and manual therapy to reduce stiffness and prevent complications like frozen joints.
2. Restoring Strength and Mobility
Muscle weakness is common after a fracture since the affected limb is often immobilised for weeks. A structured exercise program helps rebuild muscle strength and improves joint movement, ensuring a full return to normal function.
3. Preventing Muscle Wasting (Atrophy)
When a limb is immobilised, muscles start shrinking due to lack of use. Physiotherapy introduces safe, progressive exercises to maintain as much muscle strength as possible during healing.
4. Improving Balance and Coordination
For fractures affecting the legs or hips, balance and coordination can be compromised. Physiotherapists provide targeted exercises to restore stability, reducing the risk of future falls.
5. Managing Pain Without Relying on Medication
Physiotherapy techniques such as manual therapy, ice/heat therapy, and specific exercises help manage pain naturally, reducing the need for long-term medication use.
6. Gradual Return to Sports or Daily Activities
For athletes or active individuals, jumping back into sports too soon can lead to re-injury. Physiotherapists create a personalised return-to-sport plan to ensure safe participation without setbacks.

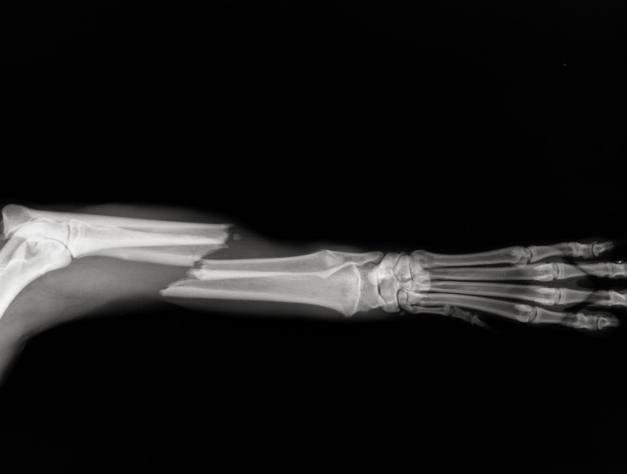
Patient Case Study: Matt’s Recovery from a Tibial Fracture
Matt, a 42-year-old mountain biker, suffered a tibial (shin bone) fracture after a high-speed crash. He underwent surgery to stabilise the bone with screws and a plate. After six weeks in a cast, Matt came to our clinic for physiotherapy, he was referred by his surgeon who wanted us to fit a knee range of motion brace and begin treating the stiffness, weakness, pain and difficulty with walking.
Matt’s Physiotherapy Journey
- Early Stage (Weeks 6-8):
- Transition from a cast to a knee range of motion brace, where we could begin to increase his available knee joint range of motion
- Gentle range-of-motion exercises to restore knee, ankle and mobility.
- Light weight-bearing exercises to gradually reintroduce walking with use of canadian crutches.
- Swelling management using ice therapy and compression.
- We used a Transcutaneous electrical nerve stimulation (TENS) machine also at this time as Matt was not keen on taking medication
- Mid-Stage (Weeks 9-12):
- Strength training with resistance bands, gym equiptment and body weight exercises. (Such as leg press, knee extension machine, hamstring curl machine, calf raise machine, hip abduction/ adduction machine).
- Gait retraining to correct his walking pattern.
- Proprioceptive exercises to improve balance and coordination. We used an aqua bag in various positions to challenge Matt.
- Advanced Stage (Weeks 13-20):
- Progressive loading exercises, including heavy squats, legpress and lunges. The goal was for Matt to achieve 1.8x his body weight for a smith machine back squat and also on a single limb leg press machine.
- Return-to-sport drills tailored to mountain biking, focusing on endurance and agility.
- Plyometric exercises to rebuild explosive power and confidence in his leg.
By the five-month mark, Matt was back on his mountain bike, riding with confidence and no lingering pain. His commitment to physiotherapy allowed him to regain full function and prevent future complications.

Tips for a Smooth Fracture Recovery
If you’ve suffered a fracture, here are some key tips to optimise your recovery:
- Follow your doctor’s advice – Adhere to weight-bearing restrictions and don’t rush the healing process.
- Stick to your physiotherapy program – Consistency is key for regaining strength and mobility. Did you know, that by doing strength training on your opposite (unaffected) limb, you will gain 15% of strength on your affected limb. Under the guidance of your physiotherapist, you should still continue to maintain your conditioning whilst your fracture is healing to reduce the amount of rehabiliation you will need to do once the bone fracture has healed.
- Eat a nutrient-rich diet – Calcium, vitamin D, and protein support bone healing.
- Get Enough Sleep – Sleeping is crucial for our bodies to repair, skipping this could lead to a longer recovery.
- Stay active within safe limits – Movement helps prevent stiffness and muscle loss.
- Be patient – Healing takes time, but with the right approach, you’ll get back to doing what you love.
- Don’t smoke – the research has shown that smoking inhibits our body to heal, therefore vaping or smoking cigarettes is going to set your recovery back.

Final Thoughts
Bone fractures can be frustrating, but with the right rehabilitation approach, you can recover fully and regain strength, mobility, and confidence. Physiotherapy plays a critical role in ensuring a safe and effective recovery, helping you return to daily activities and sports without complications. If you or someone you know has suffered a fracture, reach out to one of our physiotherapists to kickstart the healing journey. Call us on 9806 3077 today.
References and Further Reading
- Australian Physiotherapy Association – www.physiotherapy.asn.au
- Better Health Channel – Fractures – www.betterhealth.vic.gov.au
- The Bone & Joint Journal – www.bjj.boneandjoint.org.uk
- Sports Medicine Australia – www.sma.org.au
- Our Clinic’s Blog – Recovery from Fractures – www.ourclinic.com.au/fracture-recovery
Osgood–Schlatter disease (OSD) is a prevalent overuse injury affecting the knee, particularly common among active children and adolescents aged 8 to 15 who participate in sports involving frequent running and jumping, such as soccer, basketball, and athletics. This condition arises due to repetitive stress on the patellar tendon where it attaches to the tibia (shinbone), leading to inflammation and pain at the tibial tuberosity—the bony prominence just below the kneecap.
Common Symptoms:
- Pain and tenderness below the kneecap
- Swelling around the tibial tuberosity
- Pain that intensifies with physical activities like running, jumping, or kneeling
- Development of a noticeable bony lump beneath the kneecap
Diagnosis:
Healthcare professionals diagnose Osgood–Schlatter disease based on a child’s medical history, reported symptoms, and a physical examination. Typically, imaging tests like X-rays are unnecessary unless there’s a suspicion of other conditions. During the examination, the clinician will assess tenderness over the tibial tuberosity, inquire about recent growth spurts and sports involvement, and evaluate the knee’s range of motion and muscle flexibility.

Physiotherapy Management:
Physiotherapy is instrumental in managing Osgood–Schlatter disease , aiming to reduce pain, enhance flexibility, and strengthen the muscles surrounding the knee, thereby allowing continued participation in activities with minimal discomfort. Key physiotherapy strategies include:
- Activity Modification: Temporarily reducing or altering high-impact activities to alleviate stress on the knee.
- Stretching and Strengthening Exercises: Focusing on the quadriceps, hamstrings, and gluteal muscles to support knee function.
- Taping and Bracing: Utilising supportive devices to decrease strain on the tibial tuberosity.
- Pain Management: Applying ice packs to the affected area and educating on appropriate rest periods.

Exercise Program for Osgood–Schlatter Disease:
A structured exercise regimen that balances flexibility and strengthening exercises can be beneficial. It’s advisable to perform flexibility exercises daily and strengthening exercises every other day to prevent overloading. Here’s a sample program:
| Day | Flexibility Exercises | Strengthening Exercises |
|---|---|---|
| Monday | Quadriceps Stretch, Hamstring Stretch, Calf Stretch | Wall Squats, Step-Ups |
| Tuesday | Quadriceps Stretch, Hamstring Stretch, Calf Stretch | — |
| Wednesday | Quadriceps Stretch, Hamstring Stretch, Calf Stretch | Lunges, Glute Bridges |
| Thursday | Quadriceps Stretch, Hamstring Stretch, Calf Stretch | — |
| Friday | Quadriceps Stretch, Hamstring Stretch, Calf Stretch | Step-Ups, Bulgarian Split Squat |
| Saturday | Quadriceps Stretch, Hamstring Stretch, Calf Stretch | — |
| Sunday | Quadriceps Stretch, Hamstring Stretch, Calf Stretch | Banded Crab Walk, Lunges |
Note: Ensure each exercise is performed with proper form. Consulting a physiotherapist before starting the program is recommended.

Continued Participation in Sports:
Children with Osgood–Schlatter disease don’t necessarily need to cease all sports activities. However, modifying activity levels to reduce knee strain is crucial. Physiotherapists can provide guidance on maintaining physical activity while minimizing pain. Recommendations include:
- Temporarily reducing high-impact activities.
- Engaging in low-impact sports such as swimming or cycling.
- Using knee taping or braces for additional support during activities.
Prognosis:
Osgood–Schlatter disease is generally a self-limiting condition, meaning it often resolves as the child completes their growth phase. Symptoms can persist for several months but typically improve within 12 to 24 months. If pain is severe, limits daily activities, persists beyond two years, or if there’s a significant enlargement of the bony lump below the knee, further medical evaluation is warranted.
At our clinic, we recently treated a young rugby union player named Luca, who was experiencing knee pain due to Osgood-Schlatter Disease (OSD). Despite the discomfort, Luca was eager to return to the field as soon as possible.
Example Patient:
Initial Assessment:
Luca presented with classic Osgood–Schlatter disease symptoms, including tenderness and swelling just below the kneecap, exacerbated by physical activity. Understanding his commitment to rugby, we aimed to develop a treatment plan that would facilitate a swift yet safe return to play.
Treatment Plan:
- Activity Modification: We advised Luca to rest from high-impact activities for one week to reduce inflammation.
- Strapping Technique: To support the affected area and alleviate pain during movement, we applied a specific strapping technique designed for kneecap maltracking and OSD. This method involves:
- – Cutting a strip of K tape 6 cm plus the width of the patients knee
- – Cutting a second strip which is onlt 4 cm plus the wirth of the knee
- – The longer piece is used to lift the kneecap up towards the hip – applied with tension, forming a ‘U’ Shape
- – The shorter piece is applied on the outside of the knee which is applied towards the inside of the knee, bringing the knee cap inwards with tension.
- This technique provides immediate pain relief and supports the knee during activity.
- Parental Involvement: We recorded the strapping procedure and provided Luca’s parents with the video, ensuring they could replicate the technique for future games.
Outcome:
After a week of rest and consistent application of the strapping technique, Luca returned to rugby with minimal discomfort. The support from the tape allowed him to participate fully while safeguarding his knee from further strain.
Conclusion:
Luca’s case highlights the effectiveness of tailored treatment plans and the importance of involving family members in the management process. With appropriate care and support, young athletes like Luca can continue to engage in the sports they love while managing conditions like Osgood–Schlatter disease.
For a visual guide on a similar strapping technique used, you can refer to this instructional video:
Final words:
Osgood–Schlatter disease, while common among active youth, can be effectively managed through appropriate physiotherapy interventions, allowing children to continue participating in sports with minimal discomfort. If your child experiences persistent knee pain, consulting a physiotherapist is a prudent step toward recovery. Feel free to give us a call today on (02) 9806 3077
References & Further Reading:
- Osgood-Schlatter Disease – StatPearls – NCBI Bookshelf
- Osgood-Schlatter Disease (Knee Pain) – OrthoInfo – AAOS
- Osgood-Schlatter Disease: Exercises – MyHealth Alberta
- Osgood-Schlatter Disease Treatment & Management – Medscape
- Long-term Prognosis and Impact of Osgood-Schlatter Disease – PMC
- Activity Modification and Knee Strengthening for Osgood-Schlatter Disease – PMC
- Surgical Treatment Outcomes of Unresolved Osgood-Schlatter Disease – Wiley Online Library
- Osgood-Schlatter Disease: Appearance, Diagnosis and Treatment – MDPI
- Incidence and management of Osgood–Schlatter disease in general practice – BJGP
- Osgood-Schlatter Disease: A Case Report – JCM Images Case Reports